Bone Scintigraphy
A bone scan or bone scintigraphy is a scanning test to find abnormalities in bone. It is primarily used to help diagnose a number of conditions relating to bones, including: cancer of the bone or cancers that have spread (metastasized) to the bone, locating some sources of bone inflammation (e.g. arthritis, bone pain such as lower back pain due to a fracture), the diagnosis of fractures that may not be visible in traditional X-ray images, and the detection of damage to bones due to certain infections and other problems
Nuclear medicine bone scans are one of a number of methods of bone imaging, all of which are used to visually detectbone abnormalities. Such imaging studies include magnetic resonance imaging (MRI), X-ray computed tomography(CT) and in the case of 'bone scans' nuclear medicine. However, a nuclear bone scan is a functional test: it measures an aspect of bone metabolism or bone remodeling, which most other imaging techniques cannot. The nuclear bone scan competes with the FDG-PET scan in seeing abnormal metabolism in bones, but it is considerably less expensive

Nuclear bone scans are not to be confused with the completely different test often termed a "bone density scan,"DEXA or DXA, which is a low-exposure X-ray test measuring bone density to look for osteoporosis and other diseases where bones lose mass, without any bone-rebuilding activity. The nuclear medicine scan technique is sensitive to areas of unusual bone-rebuilding activity because the radiopharmaceutical is taken up by osteoblast cells that build bone. The technique therefore is sensitive to fractures and bone reaction to infections and bone tumors, including tumor metastases to bones, because all these pathologies trigger osteoblast activity. The bone scan is not sensitive to osteoporosis or multiple myeloma in bones; therefore, other techniques must be used to assess bone abnormalities from these diseases
Technique

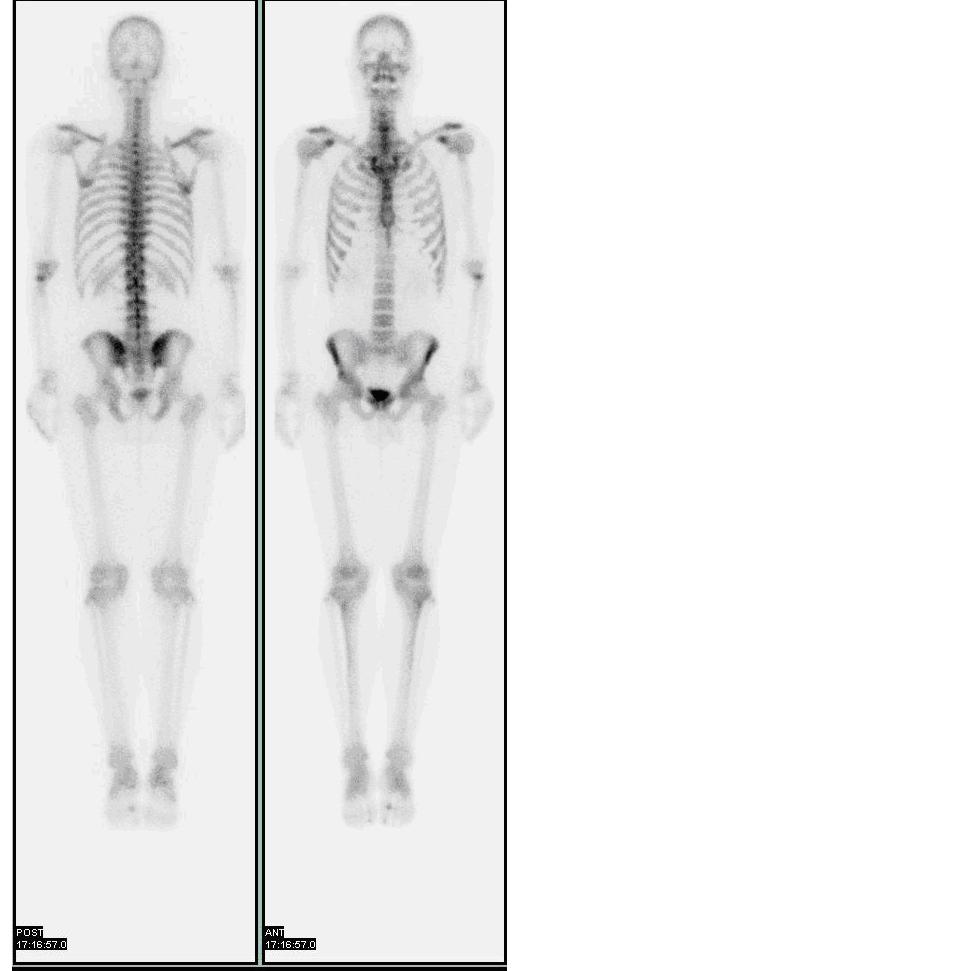
Bone scan showing multiple bone metastases from prostate cancer
In the nuclear medicine technique, the patient is injected (usually into a vein in the arm or hand, occasionally the foot) with a small amount of radioactive material such as 500 MBq of technetium-99m-MDP and then scanned with agamma camera, a device sensitive to the radiation emitted by the injected material. Two-dimensional projections ofscintigraphy may be enough, but in order to view small lesions (less than 1 cm) especially in the spine, single photon emission computed tomography (SPECT) imaging technique may be required. A disruption of bone turnover by a pathologic process on the order of 5 to 15% from normal can be detected by bone scintigraphy. Specificity of bone scintigraphy can be increased by performing an labeled white blood cell test combined with a technetium-99m-MDP injection
About half of the radioactive material is localized by the bones. The more active the bone turnover, the more radioactive material will be seen. Some tumors, fractures and infections show up as areas of increased uptake. Others can cause decreased uptake of radioactive material. Not all tumors are easily seen on the bone scan. Some lesions, especially lytic(destructive) ones, require positron emission tomography (PET) for visualization
About half of the radioactive material leaves the body through the kidneys and bladder in urine. Anyone having a study should empty their bladder immediately before images are taken
In evaluating for tumors, the patient is injected with the radioisotope and returns in 2–3 hours for imaging. Image acquisition takes from 30 to 70 minutes, depending if SPECT images are required. If the physician wants to evaluate for osteomyelitis (bone infection) or fractures, then a Three Phase/Triphasic Bone Scan is performed where 20–30 minutes of images (1st and 2nd phases) are taken during the initial injection. The patient then returns in 2–3 hours for additional images (3rd Phase). Sometimes late images are taken at 24 hours after injection
The three phase bone scan detects different types of pathology in the bone. The first phase is also known as the nuclear angiogram or the flow phase. During this phase, serial scans are taken during the first 2 to 5 seconds after injection of the Technetium-99m-MDP. This phase typically shows perfusion to a lesion. Cellulitis shows up more in phase 1 and phase 2 scan, but not in phase 3. Pathology that is more moderate to severe will show more in the first two phases. Pathology that is chronic or partially treated will be more pronounced in the third phase of a triphasic scan
The second phase image, also known as the blood pool image is obtained 5 minutes after injection. This shows the relative vascularity to the area. Areas with moderate to severe inflammation have dilated capillaries, which is where the blood flow is stagnant and the radioisotope can "pool". This phase shows areas of intense or acute inflammation more definitively compared with the third phase
The third phase, delayed phase, is obtained 3 hours after the injection, when the majority of the radioisotope has been metabolized. This phase best shows the amount of bone turnover associated with a lesion

Person undergoing a bone scan on the skull
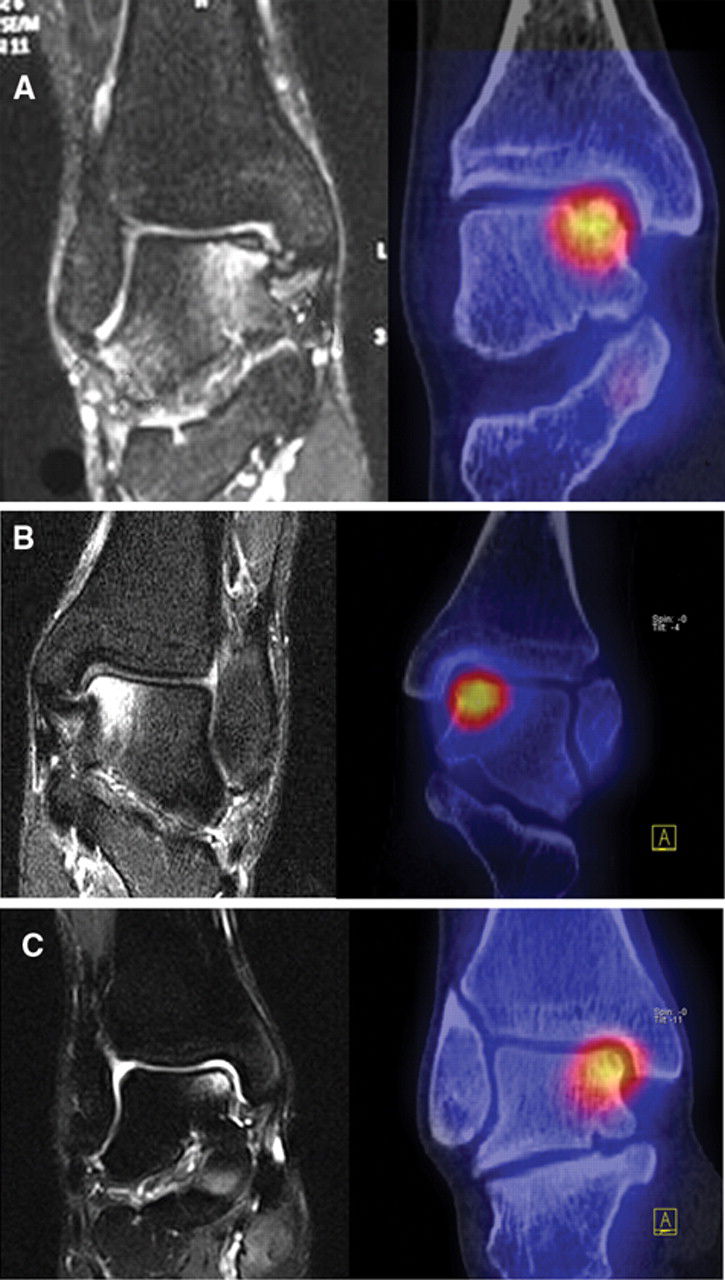
SPECT and SPECT/CT more precisely localizes tracer abnormalities in the bones compared to static imaging alone. The greatest value lies in the accurate localization of affected regions in complicated cases and small bone structures. (see below image)
Radiation Exposure
A typical radiation dosage obtained during a bone scan is very low 3.3 mSv
Dr. Ibrahim Al Butaihi
Consultant Nuclear Medicine